Dysport Training & Certification Course
- Sep 02, 2024
- | 27

Introduction
Dysport® Injection Training Course Certification (abobotulinumtoxin A) | Video Instructions
Dysport Certification Training (abobotulinumtoxin A)
History of Botulinum Neurotoxin A
In 1950, researchers at McGill discovered that botulinum toxin from the bacterial Clostridium botulinum presynaptically blocked the release of acetylcholine from motor nerve terminals. Effect was muscle weakening due to chemical denervation. It was also discovered that botulinum toxins blocked the exocytosis of acetylcholine by enzymatically degrading portions of the soluble N-ethyl maleimide-sensitive factor attachment protein receptor proteins, also known as SNARE.
In the 1970s, Dr. Alan Scott, an ophthalmologist was seeking an alternative to surgery for the correction of strabismus. He published his first study using his formulated botulinum toxin called “Oculinum” into the extraocular muscles in 1980. In 1989, onabotulinumtoxinA was FDA approved for strabismus.
In 1992, Dr. Jean Carruthers noticed an improvement in glabellar lines in patients treated with Oculinum, and published the first clinical trial for its cosmetic use. Then in 2002, Botox Cosmetics, or onabotulinumtoxinA, was approved for the use on the glabellar lines. Dysport, or abobotulinumtoxinA was FDA approved in 2009 for use on the glabellar lines.
Science of Botulinum Neurotoxin A
Botulinum neurotoxins are biological products, synthesized by bacteria, and purified for therapeutic use. Seven different serotypes of botulinum toxins occur in nature (types A through G), but most clinical products are based on the A serotype. Myobloc is the only botulinum toxin product that is based on serotype B. Botulinum toxin type A reduces acetylcholine release from motor nerves and inhibits muscular contractions at the neuromuscular junction.
The doses of botulinum neurotoxins are expressed in units of biological activity. These units are not interchangeable among different botulinum neurotoxin products. The onset of effect can occur within 24 hours. The benefit can last at least up to 4 months.
What is Dysport?
Dysport is an acetylcholine release inhibitor and a neuromuscular blocking agent. It is FDA approved and indicated for the temporary improvement in the appearance of moderate to severe glabellar lines associated with procerus and corrugator muscle activity in adult patients less than 65 years of age. Other off label use includes horizontal forehead lines and crow’s feet.
After injection, the facial muscles cease to move, and the wrinkles will diminish. Patients will begin to see effects of muscle relaxation within several days, taking up to 5 – 7 days to see full effect. Relaxation of the muscle due to Dysport® can last up to 3 – 4 months. Rarely up to 6 months.
A common misconception is that Dysport® is used to fill lines. DYSPORT® is not a type of Dermal Filler. It does not fill in lines. It relaxes muscles. DYSPORT® also does not numb your face as it affects the neuromuscular junction.
Dysport Mechanism of Action
Dysport inhibits release of the neurotransmitter, acetylcholine, from peripheral cholinergic nerve endings. Toxin activity occurs in the following sequence: Toxin heavy chain mediated binding to specific surface receptors on nerve endings, internalization of the toxin by receptor mediated endocytosis, pH-induced translocation of the toxin light chain to the cell cytosol and cleavage of SNAP25 leading to intracellular blockage of neurotransmitter exocytosis into the neuromuscular junction. Recovery of transmission occurs gradually as the neuromuscular junction recovers from SNAP25 cleavage and as new nerve endings are formed.
Comparison of Botulinum Toxins
Botox® (onabotulinumtoxinA), Dysport®(abobotulinumtoxinA) and Xeomin®(incobotulinumtoxinA) are the three FDA approved botulinum toxins for the treatment of glabellar lines in the USA. The botulinum neurotoxin molecule is a single chain polypeptide, but the formulations vary in the presence of complex proteins. Botox® contains a larger number of complexing proteins than Dysport®. Xeomin® does not contain any complexing proteins in the formulation. It is generally believed that the dosing ratio between Botox®: Dysport® : Xeomin® is around 1 : 2.5 : 1 (meaning 1 unit of Botox = 2.5 units of Dysport = 1 unit of Xeomin). It is paramount that you understand the appropriate dilution during your Dysport certification training so that your patients do not get over or under dosed.
All three products have similar safety profiles. Botox® and Dysport® must be kept refrigerated, but Xeomin® may be stored at room temperature due to its high stability. All three products recommend using nonpreserved saline.
However, studies have suggested preserved saline, which contain benzyl alcohol, can be used without affecting the potency of botulinum toxin.Also, prescribing information on all three products recommend discarding if not used within 4 hours, but studies have shown no decrease in efficacy for months after reconstitution when the product was refrigerated.
Also, prescribing information on all three products recommend discarding if not used within 4 hours, but studies have shown no decrease in efficacy for months after reconstitution when the product was refrigerated.
Reconstitution with a larger volume of saline may cause a greater diffusion of the product, which may cause unwanted adverse effects. Also, a concentrated solution is less painful to the patient.
Research has shown that Dysport displayed significantly longer duration of action than Botox. Dysport also appeared to have a faster onset of action and less injection pain than Botox.
Clinical Study

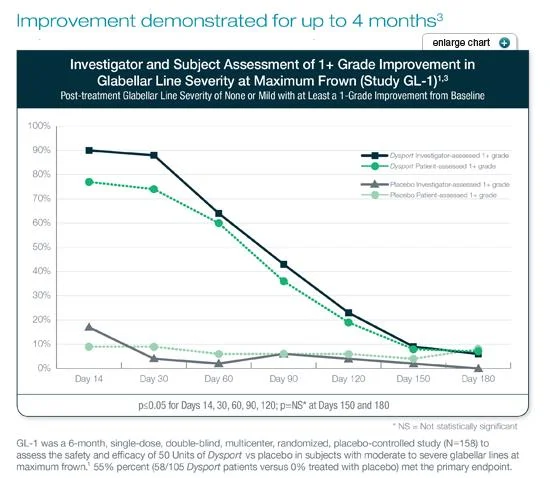
Three double-blind, randomized, placebo-controlled, clinical studies evaluated the efficacy of Dysport® for use in the temporary improvement of the appearance of moderate to severe glabellar lines. These 3 studies enrolled healthy adults (ages 19—75) with glabellar lines of at least moderate severity at maximum frown. Subjects were excluded if they had marked ptosis, deep dermal scarring, or a substantial inability to lessen glabellar lines, even by physically spreading them apart. The subjects in these studies received either Dysport or placebo. The total dose was 50 units delivered in equally divided aliquots to specified injection sites.
Additional endpoints for each of the studies were post-treatment glabellar line severity of none or mild with at least a 1-grade improvement from baseline for separate investigator and subject assessments at Day 30.
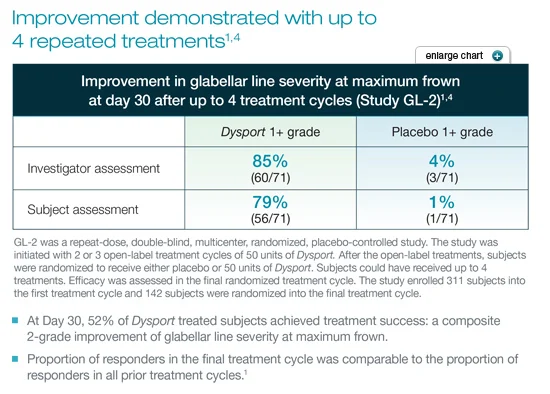
Studies GL-1 and GL-3 were 6- and 5-month (respectively) single-dose studies comparing Dysport to placebo. GL-2 was a study of Dysport vs placebo in subjects who had received up to 4 treatments of Dysport over the course of the study.
Demonstrated Results
Repeatable Results
CONTRAINDICATIONS
Dysport is contraindicated in patients with known hypersensitivity to any botulinum toxin preparation or to any of the components in the formulation. This product may contain trace amounts of cow’s milk protein. Patients known to be allergic to cow’s milk protein should not be treated with Dysport. Dysport is contraindicated for use in patients with infection at the proposed injection site(s).
Ingredients in Dysport
Active ingredient: (botulinum toxin Type A)
Inactive ingredients: human albumin, and lactose. Dysport may contain cow’s milk protein.
DOSAGE AND ADMINISTRATION
The potency Units of Dysport are specific to the preparation and assay method utilized. They are not interchangeable with other preparations of botulinum toxin products and, therefore, units of biological activity of Dysport cannot be compared to or converted into units of any other botulinum toxin products assessed with any other specific assay method.
WARNINGS AND PRECAUTIONS
Facial Anatomy in the Treatment of Glabellar Lines
Caution should be exercised when administering Dysport to patients with surgical alterations to the facial anatomy, excessive weakness or atrophy in the target muscle(s), marked facial asymmetry, inflammation at the injection site(s), ptosis, excessive dermatochalasis, deep dermal scarring, thick sebaceous skin or the inability to substantially lessen glabellar lines by physically spreading them apart.
Do not exceed the recommended dosage and frequency of administration of Dysport. In clinical trials, subjects who received a higher dose of Dysport had an increased incidence of eyelid ptosis.
Pre-existing Neuromuscular Disorders
Individuals with peripheral motor neuropathic diseases, amyotrophic lateral sclerosis or neuromuscular junction disorders (e.g., myasthenia gravis or Lambert-Eaton syndrome) should be monitored particularly closely when given botulinum toxin.
Patients with neuromuscular disorders may be at increased risk of clinically significant effects including severe dysphagia and respiratory compromise from typical doses of Dysport.
Human Albumin
This product contains albumin, a derivative of human blood. Based on effective donor screening and product manufacturing processes, it carries an extremely remote risk for transmission of viral diseases.
A theoretical risk for transmission of Creutzfeldt-Jakob disease (CJD) is also considered extremely remote. No cases of transmission of viral diseases or CJD have ever been reported for albumin.
Intradermal Immune Reaction
The possibility of an immune reaction when injected intradermally is unknown.
Drug Interactions

Patients treated concomitantly with botulinum toxins and aminoglycosides or other agents interfering with neuromuscular transmission (e.g., curare-like agents) should be observed closely because the effect of the botulinum toxin may be potentiated. Use of anticholinergic drugs after administration of Dysport may potentiate systemic anticholinergic effects such as blurred vision.
The effect of administering different botulinum neurotoxin products at the same time or within several months of each other is unknown. Excessive weakness may be exacerbated by another administration of botulinum toxin prior to the resolution of the effects of a previously administered botulinum toxin. Excessive weakness may also be exaggerated by administration of a muscle relaxant before or after administration of Dysport.
USE IN SPECIFIC POPULATIONS
Dysport is not recommended for use in children or pregnant women.
Spread of Toxin Effects: In some cases, the effects of Dysport and all botulinum toxin products may affect areas of the body away from the injection site. These effects can cause symptoms of a serious condition called botulism. Symptoms of botulism can happen within hours, or days to weeks after injection and may include swallowing and breathing problems, loss of strength and muscle weakness all over the body, double vision, blurred vision and drooping eyelids, hoarseness or change or loss of voice, trouble saying words clearly, or loss of bladder control. Swallowing and breathing problems can be life threatening and there have been reports of death.
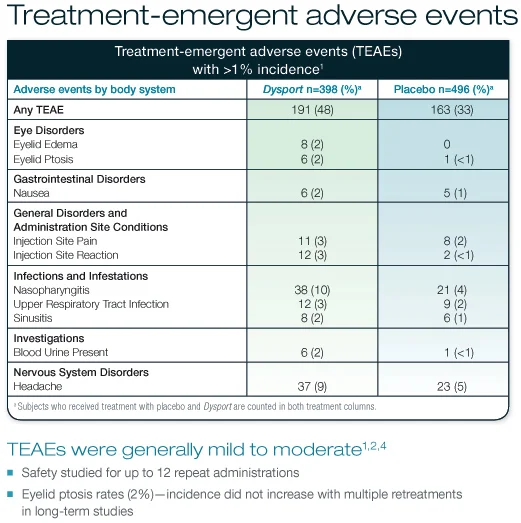
ADVERSE REACTIONS
In clinical studies, the most frequently reported adverse events (>2%) were nasopharyngitis, headache, injection site pain, injection site reaction, upper respiratory tract infection, eyelid edema, eyelid ptosis, sinusitis, nausea, dry mouth, tiredness, neck pain, and muscle pain. You should watch out for signs of eye problems: double vision, blurred vision, decreased eyesight, problems with focusing the eyes (accommodation), drooping eyelids, swelling of the eyelids Symptoms of an allergic reaction to Dysport may include: itching, rash, red itchy welts, wheezing, asthma symptoms, or dizziness or feeling faint.
Immunogenicity Information
As with any therapeutic proteins, there is a potential for immunogenicity.
The incidence of antibodies among products in this class varies depending on the sensitivity and specificity of the assay. Comparisons of the incidence of antibodies across products in this class may be misleading.
There was no evidence of neutralizing antibodies in 1,554 clinical study patients who received up to nine treatment cycles of Dysport for the treatment of moderate to severe glabellar lines.
Two subjects (0.13%) tested positive for binding antibodies at baseline, and three additional patients tested positive for binding antibodies after receiving Dysport treatment. None of the patients tested positive for neutralizing antibodies.
Patient Consultation
Always start with a through history, informed consent and a photo to document the patient’s “before” status. Provide a mirror and ask the patient what area or feature of the face is bothering him or her. Ask them to animate their face to illustrate their concerns. Evaluate your patient’s face for asymmetry and point them out to your patient, as well as documenting it on the medical record.
Set realistic expectations and educate your patient depending on your analysis of that individual. Setting unrealistic expectations will eventually lead to high patient dissatisfaction. Proper patient selection and education is paramount to a patient’s satisfaction. DYSPORT® & dermal fillers alone will not completely eliminate all the wrinkles. Some patients benefit from a face lift or a laser resurfacing procedure.
Glabellar spread test is a very useful test to see if DYSPORT® alone will soften a patient’s frown line. You spread the glabellar wrinkles apart with your thumb and index fingers. Patients with thick skin and deep dermal folds who do not improve with manual spreading will respond poorly to Dysport® injections alone. These patients require dermal filler injections. Understanding how to conduct patient consultation is a crucial skill that will be discussed during your Dyport certification training.
Reconstitution
- Dysport must maintain temperature between 36-46°F (2-8°C) to maintain viability of protein. This will be kept in refrigerator until just prior to use.
- Identify product, verify lot number and expiration date of un-reconstituted neuromodulator.
- Vigorously scrub vial tops of 0.9% NaCl (Bacterostatic) and neuromodulator with alcohol swab.
- Using sterile technique, an 18 gauge needle and 3cc sterile syringe, draw up (1.5cc) of 0.9% NaCl with Preservative. Note: Non-preservative NaCl 0.9% will be used only if the guest has an allergy to Visine products. Insert the dilutent gently and slowly into the neuromodulator vial. The vial should stay in an upright position while reconstituting.
- Record, on the vial, the date and time the bottle was reconstituted.
- Once reconstituted, the preservative reconstituted vial will remain viable for up to 2 weeks refrigerated when utilizing NaCl 0.9% with preservative and ONLY 8 hours when utilizing Preservative-Free NaCl 0.9%.
- From reconstituted vial, vigorously scrub vial top with alcohol swab. Insert needle into rubber topper of vial. Gently draw up the diluted neuromodulator with injecting syringe (0.5 cc tuberculin syringe) with desired units of product to be injected. EX: 0.05ml = 10 units (Drawing up 50 units will yield 0.25ml).
Glabellar Lines

Anatomy
The glabellar complex consists of the two corrugator supercilii muscles and the procerus muscle. These muscles pull depresses and medially contract the eyebrows. The corrugator supercilii typically lie horizontally from medial eyebrow to near the mid-pupillary position. Some patients have long corrugator muscles that extend beyond that mid-pupillary line. The procerus stands vertically between the eyebrows. The frontalis muscle is a superficial muscle that elevates the brow. Please note that the frontalis overlaps the corrugator superficially. An injection placed superficially may cause paralysis of the inferior edges of the frontalis muscle. Orbicularis oculi is the thin, circular, “purse string” like muscle that surrounds the orbital rim. The levator palpebrae muscle lies underneath the bony orbital rim, and its function is eyelid opening.
Evaluation
While standing directly in front of the patient, ask your patient to look straight and frown. Visualize the corrugator and procerus muscle. Now place your noninjecting thumb and ask the patient to frown. Try to grab the corrugator with your thumb and index finger. Feel along the entire length. While the patient face is at rest, mark the mid-pupillary position on the forehead. This will serve as your marker so that your injection will not extend laterally from this mark. To steady your hand for injection, try resting your pinky on the patient’s nose or lateral hand on the patient’s cheek like a tripod. All of these techniques will be discussed during your Dysport certification training day.
Injection Technique
All injections for the Glabella are intramuscular injection perpendicular to the skin. There are five injection sites: one at each medial corrugator or above the medial cantus, one at each lateral corrugator or above the mid-pupillary position and one into the procerus muscle (just above the crossing point of an imaginary X formed by drawing a line from medial eye brow contra-lateral to the medial canthus). All injections should be 1 cm above the orbital rim to minimize the risk of eyelid ptosis. Injection too high above 1cm can also cause eyebrow ptosis in patients who use their frontalis muscle to open their eyes. The 1 cm measurement is made from the palpable boney orbital rim and not from the anatomical eyebrow. The lateral corrugator injection can be at or just medial to the mid –pupillary line (this will reduce the likelihood missing the corrugator muscle if the corrugator muscle is short).
The standard dose of Dysport for the glabellar lines is 50 units total (10 units per injection site) in women and those with small to medium muscle mass. Final dosage may vary depending on the patient’s muscle strength and desired outcome. Higher doses may be required in men or those with thick corrugator muscles. Men often have straighter brow appearance as opposed to women.
To decrease the pain of the injection, we recommend the following: use ice or apply topical numbing cream, use a small gauze needle, use preservative containing normal saline for dilution and ask patient to not contract their muscle during injection.
Adverse Events
The most common adverse events are pain at the injection site, bruising, headache, eyebrow ptosis and eyelid ptosis. Eyelid ptosis is typically caused by diffusion of botulinum toxin into the levator palpebrae muscle. This is typically from the lateral corrugator or the mid-pupillary injection. This can be minimized by ensuring that the injection is 1cm above the boney rim or protecting the orbital rim by resting the thumb of the noninjecting hand on the superior portion of the orbital rim.
Two multicenter studies show a lid ptosis rate of 5.4% and 1%. Lid ptosis can appear within 2 to 7 days. It typically resolves within 2 to 6 weeks. Iopidine 0.5%, Naphcon-A, and phenylephrine 2.5% are alpha-adrenergic agonist ophthalmic eye drops that improve the appearance of lid ptosis, as these drops stimulate the Müller’s muscle to elevate the ptotic eyelid. Typical dosage is 2 drops, BID or TID, until resolution, but no longer than 1 month. Brow ptosis can occur when the corrugators are injected superficially which causes frontalis muscle paralysis. Injection lateral to the mid-pupillary line may cause also cause brow ptosis.
Forehead Lines

Anatomy
The vertical frontalis muscle is responsible for the formation of the horizontal forehead lines (HFL). Dysport can be used off-label to smooth these wrinkles. The frontalis muscle inserts into the periocular muscles such as the procerus, corrugator supercilii, orbicularis oculi, and depressor supercilii. Superiorly, the frontalis inserts into the galea of the scalp. Often, muscle fiber will be absent in the midline of the forehead. The fibers of the frontalis muscles are oriented vertically, while the wrinkles from the frontalis mucles form horizontally.
Evaluation
While standing directly in front of the patient, ask your patient to forcefully raise the eyebrows up and visualize the lines. Note the points of maximal contraction, brow asymmetry and ptosis and discuss this with your patient. The goal for the treatment is to soften the lines without causing brow ptosis or eliminating all expression. A conservative approach is recommended, as many patients do not want a ‘frozen face’ or a droopy, heavy eyebrow. The frontal process of the zygomatic bone fuses with the frontal bone and creates a palpable ridge that an injector can feel bilaterally on the lateral forehead. Draw a line here as frontalis rarely extend laterally to this palpable ridge. Test this assumption by asking your patients to lift their eyebrow while palpating outside of this boney ridge. You will likely feel the frontalis muscle only medial to this boney ridge.
Injection Technique
Technique and injection points vary depending on the patient. Frontalis muscle shape will vary from tall, short, narrow, wide, or V-shape. Please see the figure for possible different forehead injection patterns. Also, it is important to note that a higher injection point above the mid brow is recommended to avoid flattening an arched feminine eyebrow in women. It is recommended that you inject at least 2 cm above the eyebrow (or upper 2/3 of the forehead) to minimize brow ptosis.
This also maintains a more natural appearance. Consensus recommendation by a panel of experts has suggested 4 to 6 total injection sites. The injections are subcutaneous, roughly 2 cm apart. Typical recommendation is to inject the minimal amount of dosage, 5 units of Dysport per injection site, with close follow up in2 weeks.
Many use a V-shaped configuration for injections in women to create an arched eyebrow. This should be avoided in patients who do not desire this look, such as some male patients. If your patient experiences an undesired arched eyebrow, then this can be corrected with a small dose of additional toxin (4 – 5 units) 1–2 cm superior to the apex of the arched eyebrow.
Adverse Events
Adverse events include injection site pain, bruising and swelling, headache, eyebrow ptosis, and eyelid ptosis. Patients with advanced age (over 60), mild brow ptosis at baseline and hyperfunctional eyebrow (patients who use their frontalis muscle to open their eyes) should be treated with caution. Treatment of the glabellar muscles will minimize the eyebrow ptosis.
Crow’s Feet

Anatomy
Eyelid skin is thin and elastic, with no underlying subcutaneous fat. Orbicularis oculi, is an elliptical muscle that closes the eyelids and acts as the sphincter of the eye. Orbicularis oculi has three parts: orbital, palpebral and lacrimal. The lacrimal part connects to the lacrimal sac and inserts on the upper and lower eyelids at the tarsal plate. The palpebral part is the innermost aspect of the muscle and provides the less forceful closure of the eyelid, such as a blink. The orbital part is outermost aspect of the muscle and blends into the surrounding muscles. This is part that accounts for the forceful closure of the eyelids and pulls the skin. Zygomaticus minor typically lies deep to the orbicularis oculi from the zygomatic bone. Therefore, a deep injection should be avoided here. Dysport (an off-label use) can be injected into the orbicularis oculi for treatment of crow’s feet.
Evaluation
The lateral portion of the orbicularis oculi lies in a vertical direction. Researchers have identified up to 4 different lateral canthal rhytid patterns. A standard injection points are taught to beginners, but in some instances, treatment may require individualization. Evaluate the crow’s feet by asking the patient to squint. Note any asymmetry, lid ptosis, brow ptosis, scleral show or lid laxity. Most importantly, use bright light and stretch the skin to find any fine vessels coursing through this region and mark them to avoid an injection into them.
If you feel that your ideal injection mark is immediately over a vessel, then place you injection lateral to the vessel. Also we recommend that you mark the palpable lateral orbital rim. This will aid in ensuring that your injection is placed outside of the boney rim. Finally, discuss with your patients other adjunctive treatment options such as various skin tightening modalities to improve patient satisfaction.
Injection Technique
Dysport for Crow's Feet Injection Demonstration | Dysport Training
Stand in a position so that the needle is pointed away from the eye (inject superiorly, needle pointing up to the ceiling). You may use your noninjecting finger to shield the globe by placing your index finger in the lateral orbital groove or stretch the skin to aid in the penetration of the skin. Injections should be superficial dermal injections(2 – 3 mm deep) resulting in a wheel formation. Injections are also commonly 1.5cm from the lateral canthus or 1cm lateral to the boney orbital rim. Dysport is injected 1 to 1.5 cm apart in an arc-like pattern using 8 units per injection. Place your middle injection lateral in-line with the lateral canthus.
Adverse Events
Similar adverse events such as pain and swelling can occur. Rate of ecchymoses can be high at 25%. This can be avoided by injecting around a vessel, superficially with only the tip of the needle in the skin. Pressure should be applied immediately for up to 5 minutes to reduce the risk of a hematoma. Lip ptosis can rarely occur due to involvement of the lip elevator muscles that blend with the orbicularis oculi muscle.
The rate of this complication is less than 1%, and is due to deeply or inferiorly placed injections. No treatment is available, but it is reported that the muscle normalizes within 6 weeks. Some patients may notice a new wrinkle beneath the eye or along the malar prominence, especially when smiling. This may be due to the contraction of the zygomaticus muscles and elevation of the cheek. Eyelid and eyebrow ptosis can occur if the injection diffuses into muscles above the orbital rim.
Treatment Failure
Treatment failure can be differentiated into Primary and Secondary nonresponders.
Primary nonresponders are first time Dysport® users;
- A major reason for this is due to the fact that wrinkles are not dynamic in origin (usually due to photodamage or age-related). These wrinkles had a static component to them that required the injection of a filler material.
- Injection amount may have been inadequate. This is like due to either the patient has strong muscles or your injection missed the targeted muscle.
- Toxin had denatured. Rarely, you will get a bad vial of Dysport. In this case contact your representative for replacement vial.
Secondary nonresponders
These patients initially responded to Dysport® but lose the response on subsequent injections;
- Injection amount was inadequate. This is like due to either the patient has strong muscles or your injection missed the targeted muscle.
- Toxin had denatured.
- Your patient may have developed neutralizing antibodies. This is a rare, but a side effect. You may find success in using a different Botulinum Toxin such as Myobloc on these patients.
Conclusion
- Use your hands. Feel the face. Inject where you can feel the muscle that causes the visible wrinkles.
- Always inject a relaxed face, not a face where the muscle is contracted. A contracted face distorts your landmarks and increases pain.
- Use a marking pen or a white eyeliner pencil for marking your injection site until you become proficient. Place the marks below where you will inject. Or, your injection should be above the mark. Injecting into a mark on the face can cause a tattoo on somebody.
- Remember that many landmarks are BONEY landmarks. Do not simply use surface skin landmarks as your reference.
- All complications may be seen immediately or as late as 7 days. Complication may persist for up to 4 – 8 weeks.
- Most complications are almost always temporary. In your practice, you are likely to experience a complication. Be prepared for it. Good customer service and patient reassurance that the complication is temporary will appease most patients.
- ALWAYS obtain before photos and after photos. This is an essential documentation to have to resolve any complaints.
- Reinjection should be done no earlier than one week after the first injection if the patient perceives no desire effect. Sometimes, it takes a week until a patient sees the effects.
- Application of topical EMLA anesthetic or cold ice pack will help alleviate patient discomfort and injection fears.
- Please become familiar with the Pre and Post injection instructions. Your patients will ask you about them. Also, your patient’s compliance with them will reduce complications.
- Most importantly, be conservative. You can always inject more Dysport. But, you can’t take it out.
- Practice on as many patients as possible during your onsite hands-on Dysport certification training day.
- You can set up your Dysport account using this link.
Restylane®️/Perlane®️ Injection Training Certification
Learn more about Restylane®️/Perlane®️ Injection Training Certification.
Cosmetic Medical Training recognizes that many of the techniques and recommendations for this Dysport Certification Training text are considered off-label use. Our recommendations are based on many textbooks, published articles, seminars and practical knowledge and experience. The authors have attempted to maintain up to date knowledge and information in this training manual with the current standard of care. However, due to continuing flow of new research and information relating to the drugs being used in this course, we recommend that you check with the manufacturer for any changes in the package inserts, warnings and precautions.
Statement of Responsibility
All information and tools presented within this site are intended for educational purposes. We do not guarantee that the information will be completely accurate and up to date; therefore the authors will not be held responsible for any errors, omissions or inaccuracies published. Application of the knowledge is ultimately the responsibility of the practitioner.
The owners, authors and any participants disclaim all liability or loss in conjunction with any content provided here. We disclaim any liability for products or services recommended including defective products or direct, indirect, special, incidental or consequential damages, arising out of the use or the inability to use the materials/information published. We recommend that the user reviews the package inserts for all the drugs that are discussed within this training recommendation before use.
Originally published at Dysport Training Austin